Equine vector-borne diseases, such as piroplasmosis and anaplasmosis, are vector-borne-infections that are often responsible for similar clinical symptoms. However, these pathologies differ in their origin, geographical distribution and seasonality, making differential diagnosis essential to ensure rapid and effective treatment.
Equine piroplasmosis is caused by the protozoan parasites Babesia caballi and Theileria equi, transmitted by ticks of the genus Dermacentor, Ixodes and Rhipicephalus. When they bite, these ticks inoculate the parasites through their saliva, causing clinical signs such as hyperthermia, despondency, anaemia and hepatorenal disorders in the horse. In acute forms, the course can be fatal in less than 72 hours without appropriate treatment.
Equine anaplasmosis, on the other hand, is a bacterial disease caused by Anaplasma phagocytophilum, transmitted mainly by Ixodes ticks.
It causes symptoms similar to those of piroplasmosis, such as fever, lethargy, anorexia, limb oedema, and thrombocytopenia.
Often underdiagnosed, anaplasmosis is nonetheless present in Europe and North America, with distinct seasonal activity periods.
Piroplasmosis is widely distributed in tropical, subtropical and temperate regions, including South America, Africa, Asia and Southern Europe. It tracks tick activity, with an increased prevalence in spring and summer in temperate zones.
Anaplasmosis, on the other hand, is more common in the wooded and humid regions of Europe, North America, and Asia. Its infection cycle is bimodal, with peaks in spring and autumn, when ticks of the genus Ixodes are most active.
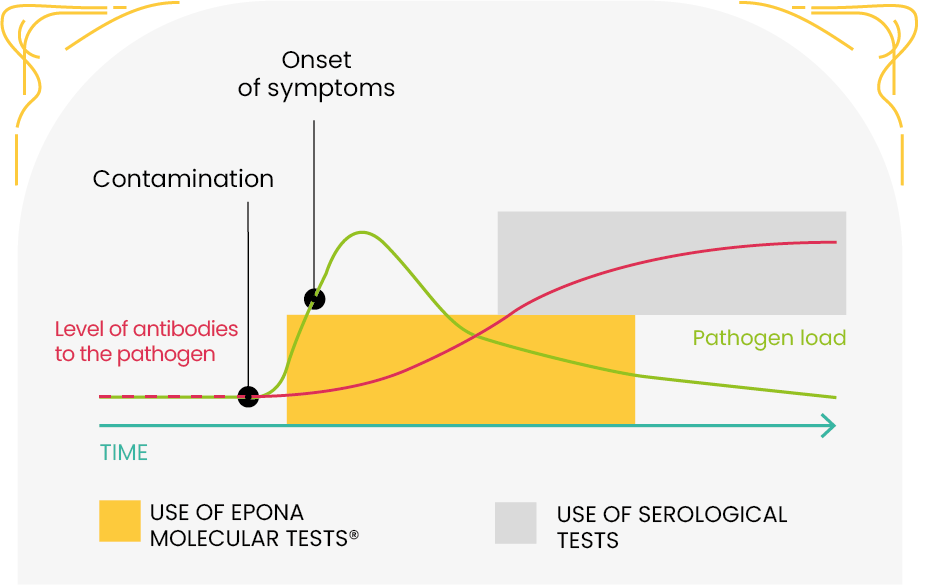
During the acute phase of infection, tick-borne diseases can be diagnosed by various methods:
For maximum effectiveness, it is recommended to combine several of these methods, as they are complementary and can detect different elements.
Imidocarb is a drug that does not have an MA for equine treatment. Its injection is very violent for the horse, leading to spams, tremor, or convulsions.
Digestive issues are frequent, and colic or vomiting must be taken seriously as they can result in fatal exhaustion. Imidocarb should therefore only be used if a positive case of piroplasmosis is established.
Anaplasmosis is often underdiagnosed and should
not be treated with Imidocarb but with antibiotics. Differentiating between piroplasmosis and anaplasmosis is essential for proper treatment.
There is no vaccine against piroplasmosis or anaplasmosis in horses, so here are some recommendations to give to your clients to avoid its occurrence:
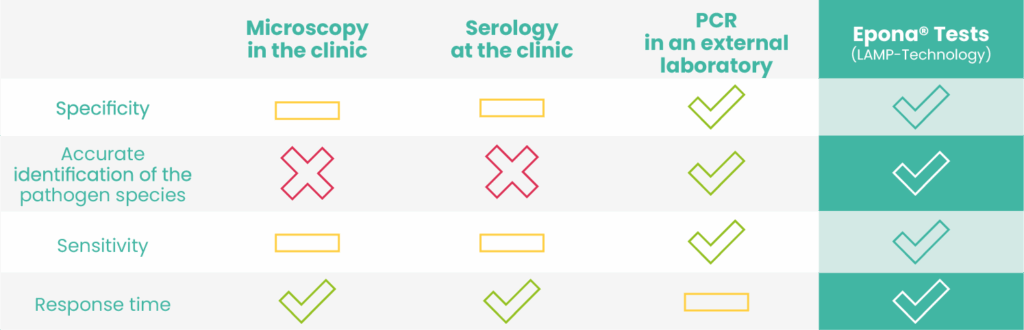
Epona® tests are molecular biology tests that directly detect the DNA of the pathogen and can therefore be used from the beginning of the infection even before symptoms are detectable.
Their sensitivity is very close to that of PCR, but the results are obtained in 30 minutes.